
 American English
American English
[showglossary gid=”1697″]
Milk Fever in Cattle
Also known as: Calcium Deficiency, Hypocalcaemia, Periparturient Paresis
Milk fever is caused by a temporary blood calcium deficiency (also known as hypocalcaemia) which usually occurs around the time of calving and is one of the most common metabolic disorder in dairy cattle. This condition is a common cause of poor labour (dystocia), stillborn calves and apparent sudden death of dairy cows.
– what is normal?
A normal plasma concentration of calcium is between 8.8 – 10.4 mg per 100 ml (2.2 – 2.6 mmol/l). In 30-40% of cows this will fall below 6.0 mg/100 ml (2.0 mmol/l) at calving. When blood calcium falls to 3-6mg per 100 ml (0.75 – 1.5mmol/l) clinical signs of milk fever will usually occur (Roche, 2003).
Some degree of hypocalcaemia occurs in all cows around calving, but only when this becomes severe do clinical signs develop. Cows only have a small amount of calcium circulating in their blood (about 10g) but they have a considerable reservoir of calcium stored in their bones (6,000g), and plenty in the food in their gut (100g). During late pregnancy and early lactation the calcium demand increases significantly, causing blood calcium levels to drop. The underlying factor around calving is the sudden increase in calcium requirements for the production of colostrum. The cow adapts to this increased demand by increasing calcium absorption from the gut and the mobilisation of calcium reserves in bone. The regulation of blood calcium level is controlled by the parathyroid hormone and the production of 1,25-dihydroxycholecalciferol from vitamin D3. (Image below)
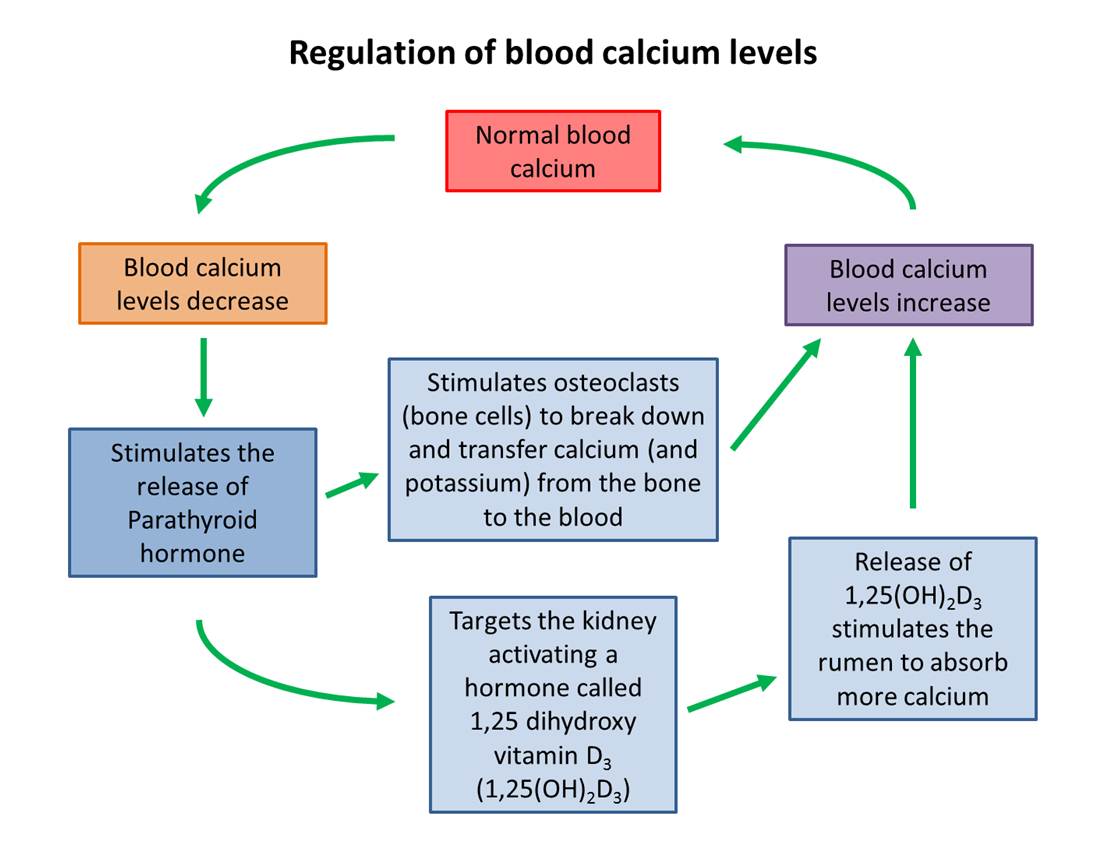
Blood calcium regulation adapted from Blowey, 2006
Factors affecting the ability of the cow to regulate the blood calcium process effectively are:
- Age of the cow – older cows are less able to mobilise calcium from the skeleton
- High levels of oestrogen around calving inhibit calcium mobilisation
- Cows eat less around calving and thus calcium intake is often reduced
- Bone resorption of calcium is inhibited in cows fed high potassium or high sodium diets as a result of metabolic alkalosis (Goff and Horst, 1997; Horst et al., 1997)
- High calcium intake during the dry period reduces the response to higher demands (Horst, 1986)
- Low magnesium intakes reduce the ability of the gut to absorb calcium (Sansom et al., 1983)
- Problems associated with digestion, such as acidosis and profuse diarrhoea, will reduce the amount of calcium available for absorption (Eddy, 1992)
The average annual incidence of clinical milk fever in dairy herds has been estimated to be about 5% (Whitaker et al., 2004), although it tends to be lower in first parity cows with the risk increasing with subsequent lactations. Subclinical hypocalcaemia can potentially have widespread effects on the cow that predispose her to other metabolic and periparturient diseases (Curtis et al., 1983). Cows with milk fever have a higher plasma cortisol concentration which may exacerbate the immunosupression normal at calving. Additionally, the loss of muscle tone in the teat sphincter and the uterus may increase the risk of mastitis, retained foetal membranes, endometritis and uterine prolapse. A reduction in appetite may exacerbate the negative energy balance after calving and increase the risk of ketosis and displaced abomasum, all of which can impact on subsequent fertility in later lactation (Chebel et al., 2004; Maizon et al., 2004).

Milk fever seems to be more apparent when dry cows are fed grass particularly during long wet spells of weather.
Hypocalcaemia appears to be more common when dry cows are fed grass, rather than conserved fodder especially during long wet spells of weather. Another predisposing factor is breed, with the Jersey and, to a lesser extent, the Guernsey being particularly susceptible to milk fever. This is probably due to the relatively high production level for small breeds. The incidence of the disease also increases with lactation number. The reason is thought to be the increasing requirement for calcium at calving as milk yield increases with each lactation, and the ability to mobilize calcium from the skeleton decreases with age (Eddy, 1992).
Hypocalcaemia is often accompanied by hypophosphataemia and hypermagnesaemia although milk fever may also be caused by a low magnesium intake, in which case there may be hypomagnesaemia.
The incidence of milk fever in organic herds has been reported as being low (Weller and Cooper, 1996) and lower than in conventional herds (Hardeng and Edge, 2001). One of the main reasons for this may be the generally lower milk yield on organic dairy farms (Pryce et al., 1999; Hardeng and Edge, 2001) and reduced use of potassium based fertilisers (Hardeng and Edge, 2001).
Control and Prevention of Milk Fever
All cases of milk fever can and should be preventable. It is not advisable to breed from cows or sires with a history of recurrent milk fever. Also, animals should be prevented from becoming overfat or having large changes in body condition score and cows should be given plenty of exercise (Chamberlain, 2003). Cows with marked body condition loss (1-1.5 points) in the dry period are at greater risk of milk fever (Kim and Suh, 2003).
Ensure the diet of cows in late pregnancy is sufficient in magnesium to maintain plasma magnesium concentrations greater than 0.85 mmol/litre (1.8 mg/ 100 ml) as this aids parathyroid hormone production and release (Sansom et al., 1983; Husband, 2005). The calcium intake during the dry period should be kept below 50 g/day (ideally below 20g/day) in order to improve the efficiency of calcium absorption and mobilization (Horst, 1986; Thilsing-Hansen et al., 2002). However, just before calving the calcium in the diet can be increased to ensure adequate calcium is available over the risk period. The main problem of implementing the low calcium principle is in formulating rations with the commonly available feeds and grass which are often relatively high in calcium (Husband, 2005).
Click here to download Dairy Co’s Body Condition Score Factsheet
It has been reported that diets high in strong cations, such as potassium and sodium, predispose cows to milk fever (Chandler, 1997; Goff and Horst, 1997; Horst et al., 1997; Olson, 1991). Considerable research has been conducted into the addition of neutralising anions to the diet to prevent hypocalcaemia. The acid-base status of the cow dictates the sensitivity of the tissues to parathyroid hormone stimulation, with metabolic alkalosis decreasing tissue responsiveness to parathyroid hormone (Goff and Horst, 2003a). Excessive dietary potassium can occur frequently in dairy cow rations and is the most important factor contributing to metabolic alkalosis (McNeill et al., 2002; Goff and Horst, 2003a). In contrast, additional chlorine and sulphur can acidify the diet and help maintain calcium homeostasis, such that some feeding strategies focus on the use of forages with moderate to low calcium, potassium and sodium with the addition of chloride and sulphate salts (McNeill et al., 2002).
Dietary Cation Anion Difference
A review of studies investigating dietary cation-anion difference (DCAD) manipulation has shown a strong correlation between lowering DCAD and reducing the risk of clinical milk fever (Charbonneau et al., 2006). The DCAD concept is an empirical hypothesis, not a physiological mechanism and there are some drawbacks to feeding dietary anions. Anionic salts are not palatable and it may be difficult to mask the taste of anionic salts unless they are incorporated with silage. In addition, they tend to concentrate in the bottom of the feed trough rations, which are composed of dry materials. It may be difficult to add enough anionic salts to correct extremely cationic diets (Olson, 1991), and in pasture-based dry cow diets, the DCAD can be very high and very variable, such that manipulation can be unpredictable (Roche, 2003a). In pasture systems, emphasising magnesium supplementation in the pre-calving period has helped to reduce the incidence of clinical milk fever (Roche, 2003b). Long-term low DCAD grazing strategies for dry cows may be appropriate in some low input farms and involves the following;
- Selecting a small area of grazing that can be left without manuring
- Harvesting grass twice yearly
- Grazing the cows on grass regrowth’s as these have the lowest potassium content (Husband, 2005).
Large doses of vitamin D3, or alphacalcidol and oral calcium supplementation have been suggested during the week before calving in conventional, high-input farming (Agger and Renney, 2004). This strategy should not be necessary if the right dry cow management is applied, additionally, these methods are labour intensive, time consuming, and less reliable.
In summary, there are important aspects of the DCAD principle applicable in low input and organic farming, but feeding a “full DCAD” diet requires a very controlled feeding regime (Total Mixed Ration) and regular close monitoring (e.g. monitoring urine pH), which may not be necessary at moderate yield levels.
Treating Milk Fever
Before attempting treatment of a cow, it may be advisable to obtain a blood sample which can be stored and analysed if required at a later stage if the cow fails to respond as expected to treatment. The treatment of choice for milk fever is slow, intravenous infusion of 8-12 g of calcium as soon as possible after the onset of clinical signs. Calcium borogluconate containing products with or without added magnesium and phosphorus are mostly used in the UK usually 400 ml of 40% calcium borogluconate. During cold weather the solution should be warmed to body temperature. Approximately 85% of cases will respond to one treatment: in many cases cows recumbent from milk fever will rise within 10 minutes of treatment and others will get up 2-4 hours later. Intravenous therapy to elevate calcium levels quickly is important to avoid downer cow syndrome, often seen when cows are treated subcutaneously (Fenwick, 1994).
The outcome of treatment of a down cow is improved with careful nursing (Huxley, 2006). It is essential to sit the cow in a sternal recumbency position and turn her so that she is lying on the side opposite to the one on which she was found. She should be turned to lie on the opposite side every two hours. Provide shelter or cover with rugs in exposed situations and ensure food and water are available at all times.
If a response is not evident by 5-6 hours, the diagnosis should be reassessed, and, if necessary, a further intravenous infusion of 8-12 g of calcium administered. Relapses of milk fever occur in 25% of cases treated. Twelve hours after treatment, all calcium administered, whether by the intravenous or subcutaneous route, has been eliminated from the body. The treatment is only a holding operation until the normal adaptation process is in full operation. Cases of relapse usually occur at 18-24 hour intervals and should be treated in the same way although it is crucial to get the cow eating as soon as possible to obtain dietary calcium. Removal of the calf may help to prevent relapses (Eddy, 1992).
Blood samples can be taken from dry cows to determine plasma magnesium and calcium levels and to assess the metabolic profile of cows in early lactation.
The cation levels of the diet may have to be determined and if the reason is found, change the diet accordingly.
It may be possible to determine bloodlines with a history of milk fever. These should not be used for breeding.
Good Practice Based on Current Knowledge
Prevention of Milk Fever
A strategy to prevent milk fever in a herd will depend on herd-specific circumstances such as the attitude and skills of the farmer and the facilities available in the production system. Prevention of metabolic disease at calving should form an important part of an integrated herd health plan for the farm:
- Do not breed from cows or sires with a history of recurrent milk fever
- Prevent animals from becoming overfat (cows should calve at BCS 2.5-3) and ensure they get plenty of exercise
- Make sure that the diet is sufficient in magnesium for cows in late pregnancy
- Avoid stress in cows
- Feed adequate long fibre to transition cows
- Ensure that the calcium intake during the dry period is below 50 g/day
- Ensure that adequate dietary calcium is available over the risk period (just prior to and after calving)
- Try to avoid diets high in strong cations, such as sodium and potassium
Treatment of Milk Fever
- Treat cases of milk fever as soon as possible with a slow intravenous infusion of 8-12 g of calcium
- Ensure the solution is warmed to body temperature in cold weather
- Sit the cow up in a sternal recumbency position and turn her so that she is lying on the side opposite to the one on which she was found and turn every 2 hours
- Massage the legs
- Protect cases from exposed weather conditions
- Remove the calf if a severe case
- Treat relapse cases as above

Comments are closed.