
 British English
British English
Cattle Diseases
Johne’s Disease in Cattle
Also known as: Mycobacterium johnei, Mycobacterium paratuberculosis, Paratuberculosis
Johne’s disease is an infectious, progressive, gastrointestinal disease that affects cattle and other ruminants, with calves becoming infected mainly during the first six months of life, or during pregnancy (Radia et al .2013). It is caused by the aerobic bacterium Mycobacterium avium paratuberculosis (MAP). MAP is thought to be unable to multiply outside a host, although the organism can remain viable for long periods in the environment, surviving for over a year in feces (Whittington et al., 2004, Lovell et al., 1944,), depending on the climate (Eppleston et al., 2014). Despite probable underreporting, (Daniels et al., 2002) the disease is widely distributed worldwide (Wolf et al., 2014) and causes substantial economic losses through death and loss of productivity during the prolonged subclinical stage. The absence of a simple, accurate diagnostic test means that the disease persists and frequently remains within herds undetected.
- The primary route of infection is by calves ingesting infected feces
- The Johne’s organism can survive in the environment for over a year
- Repeat testing of cattle over 2 years old gives the highest accuracy and likelihood of detection
- There is no treatment for Johne’s disease

The primary route of infection, is by ingestion of infected feces by youngstock.
MAP is spread via ingestion of feces and milk from infected animals and potentially via the placenta in pregnant animals and in the semen in infected bulls (Ayele et al., 2004). It is excreted by infected animals before clinical signs appear, although bacteria numbers increase once clinical signs have developed. It is believed that most infections occur during the first day of life of a calf and originate from the dam or by ingestion of feces from another cow in the calving area.
While there are several ways for a calf to get infected, Radia et al., (2013) identified the calving area as the main source of infection, with indoor calving, fecal exposure in the calf house and the calf’s time spent with the dam being the main risk factors for infections. Only in fourth place comes pooling of colostrum. It is important to prioritize this – many farmers place great emphasis on milk feeding practices, but may calves are already infected via the fecal-oral route before they are offered powdered milk or colostrum substitute.
After ingestion of infected feces or milk, MAP invades the small intestine via the lymphatic tissue in the intestinal mucosa, where it multiplies over the next 2-3 months and spreads to the draining mesenteric lymph nodes. The outcome of the infection depends on both the immune response of the infected animal and the dose of the initial infection, as well as the strain of bacteria (Shawn et al., 2006).
There is a large potential reservoir of MAP in the environment as it has been reported in a number of domestic and wildlife species including sheep, goats, rabbits, deer and cats (Palmer et al., 2005). Cattle tend not to avoid pasture contaminated with rabbit feces, therefore, theoretically, this may be a route of disease spread (Daniels et al., 2001; Daniels et al., 2003).
The main risk factor associated with Johne’s disease are:
- Buying-in cattle with the disease (Chi et al., 2002)
- The application of manure to pasture
- Access to feed by wildlife (Daniels et al., 2002)
- Recent calvings as immunity is compromised at this time (Stabel and Goff, 2004)
- There is also evidence to suggest that Jersey breed cattle may be more susceptible than other larger breeds (Jakobsen et al., 2000)
- Large herds are more at risk than small herds (Jakobsen et al., 2000)
Clinical Signs of Johne’s Disease

The course of the infection depends on the immune response of infected animals. The initial infection may be overcome, or the infection may persist for many months or years with intestinal lesions slowly progressing until they interfere with normal function. In response to chronic infection, there is thickening of the small intestine, especially the ileum, and a loss in permeability can result in a loss of plasma proteins and a failure to effectively absorb amino acids. Feces may be soft and pasty or more classically the animal may show signs of diarrhea. Some animals may become anemic, although animals are usually bright and have a good appetite until the disease reaches advanced stages, when animals become emaciated and weak. Clinical disease is normally seen in animals over two years of age.
Due to the long incubation period, disease is often subclinical and direct effects on production and welfare are often masked and hence it may appear difficult to justify large investment in control programs (Kennedy and Benedictus, 2001). The main economic loss from Johne’s infection in dairy herds is due to reduced milk production from clinically and subclinically affected cows (Chi et al., 2002), although there is also likely to be decreased fertility (an increased in the number of days not pregnant) (Johnson-Ifearulundu et al., 2000), resulting in increased culling of infected cows (Wilson et al., 1993; Ott et al., 1999).
Johne’s disease has been implicated in the development of Chrohn’s disease in humans, as it has been shown that MAP can be isolated from some lesions of Chrohn’s (Chamberlain et al., 2001). Additionally. both MAP DNA and viable MAP have been isolated from both raw and pasteurized milk from a number of countries, including the UK (Millar et al., 1996; Gao et al., 2002; Grant, 2003; O’ Reilly et al., 2004; Ellingson et al., 2005), with a prevalence of viable MAP of 3% found in US retail milk samples (Ellingson et al., 2005) and in 1/357 Irish retail samples (O’ Reilly et al., 2004). MAP has not been isolated from retail beef to date (Grant, 2006), and some researchers have failed to identify MAP from Crohn’s cases and argue that there is no evidence to support a role for MAP in the disease (Bakash et al., 2004). The consensus opinion currently is that there is insufficient evidence to prove or disprove that MAP is the cause of Chron’s (Grant, 2005). However, it would seem prudent to limit the prevalence of Johne’s disease from a public health perspective (both real and perceived risk) and from an animal health and welfare perspective as well as for simple farm economic reasons.
Controlling and Preventing Johne’s Disease
General Principles
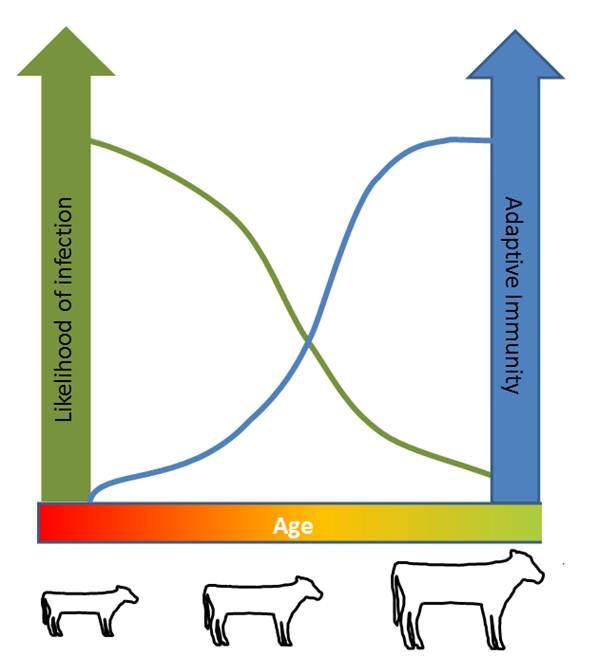
Youngstock are at highest risk of contracting Johne’s disease
Several countries (Australia, New Zealand and the USA, among others) have ongoing eradication programs for Johne’s disease (Geraghty et al. 2014). Efforts to evaluate the success of these measures have intensified recently, as concerns over the link between human Chron’s disease and consumption of MAP contaminated milk have grown. Developments in diagnostic methodologies to identify sub-clinical cases have further increased interest in planned control policies (Giessen et al., 1992; McDonald et al. 1999).
There is a general lack of data to measure the efficacy of the most frequently proposed farm level control measures and where this has been done conflicting results have been found (BCVA, 2004). However, having more than one cow in the maternity pen, group-housing pre-weaned calves in winter, and allowing beef cattle to have access to direct (nose-to-nose) contact are all factors that are significantly positively linked to the number of MAP seropositive cows (Tiwari et al., 2009).
The economic viability of control measures have been questioned (Stott et al., 2005). Management practices aiming to limit transmission via ingested feces tend to be more effective at reducing within-herd prevalence than those practices concerned with transmission via colostrum and milk (Radia et al., 2013). Improved calf hygiene strategies have been found to be the most economically attractive to farmers and may be the best control measure to limit Johne’s disease (Groenendaal and Galligan, 2003). In general, the main priorities are to identify infected herds and individuals within herds, with subsequent appropriate isolation and culling and then to focus on reducing the risk of spread of infection within and between herds.
Testing for Johne’s Disease
It is extremely difficult to be precise about disease status due to the poor sensitivity of many of the tests and the change in likelihood of obtaining a positive diagnosis with disease progression in individual animals (Jones, 2001). Many different approaches to testing have been suggested and a review of testing for Johne’s disease from a United States perspective is detailed by Collins et al. (2006).
Bulk milk ELISAs in dairy herds are too insensitive to be of any value if negative. A control program based on repeated individual milk ELISA has been described by Nielsen (2009). For beef herds a herd serum ELISA on all herd animals aged 2 years and older is a first step (BCVA, 2004; Hendrik et al., 2005). Results are most reliable for herds confirmed to be infected by isolation of MAP from at least one animal. The percentage of a herd that is ELISA-positive for MAP (apparent prevalence) should be doubled to get a rough estimate of the true prevalence of Johne’s (given a test sensitivity of roughly 50%, only half of infected animals test positive). Using the ELISA or any other test for Johne’s to estimate herd prevalence of MAP infection is only possible in herds that do not routinely test and cull test-positive animals. Prevalence of Johne’s will be underestimated by a whole herd ELISA once the cattle in advanced stages of MAP infection have been removed. Testing using the ELISA may therefore be of most value in high prevalence herds due to the low sensitivity of the ELISA test (Carpenter et al., 2004). In order to maximize the efficiency of testing for Johne’s disease it may be best to target sampling to those herds where risk assessment is deemed to be at the highest risk of disease entering (Orpin et al., 2005).
The poor sensitivity of the ELISA discussed previously may not be, in practical terms, a large a problem in relation to control (BCVA, 2004). Firstly, the prime concern in relation to control is to remove the infected animals that are shedding infection. As an increase in shedding is related to an increase likelihood of detection by ELISA (Whitlock et al., 2000) the cattle that present the greatest risk to the herd should still be detected. Secondly a test that was 100% sensitive would potentially reveal so many positives that the potential for culling all such animals may not be a viable proposition. Subsequent herd tests should occur within a year (there is some indication that annual test may provide little advantage over removing clinically diseased animals) and that six monthly testing is preferable. Testing of the herd should be continued after the cull.
Controlling Risks for Johne’s Disease Introduction and Spread

Feeding calves unpasteurized pooled waste milk results in a high risk of Johne’s disease transmission.
Taking a risk assessment based approach to a control program has been shown to reduce within-herd prevalence of Johne’s disease (Sorge et al., 2011). A risk based approach looks at current management practices and evaluates their potential to spread Johne’s disease both within, and between farms. Risk based approaches on a dairy farms in Ontario, were evaluated for effectiveness in reducing Johne’s disease. Regular testing for Johne’s disease was undertaken and assessed throughout the formulation and implementation of a control program. While the percent of herds with infected cows did not change, the average within-herd prevalence of MAP infection decreased from 5.4 to 4.2% over the two and a half year study period.
The main source of infection in a herd is via purchased stock of unknown disease status. After entering a herd, Johne’s disease tends to be cyclic, in that the disease often appears and disappears after a few years in the absence of control measures. The thick waxy cell wall of MAP renders the organism resistant to many disinfectants commonly used in agriculture. As a result, even if all infected animals are removed from a herd, MAP is likely to remain viable in the environment for many months (Jones, 2001).
Animals that have tested positive for the disease should be culled, as they pose a risk to others. Offspring born from cows that develop the disease should not be retained in the herd, as they are more likely to be infected, either from their dam’s feces or in utero. Any offspring from confirmed Johne’s cases should be fattened and sold as beef animals. Rearing heifers off site, away from infected adult cattle, has been shown to reduce the risk of Johne’s disease infection (Aly et al. 2015).
In an infected herd, calves should be removed from the dams immediately after birth and given colostrum that is known to be free of the bacteria. However, this may run counter to rearing systems where farmers wish to maximize the time the calf spends with the dam. In such circumstances, veterinary advice should be sought on the likely level of risk on an individual herd basis. Certainly in some cases early separation of calves from dams has not been shown to reduce disease (Ridge et al., 2005). On-farm batch pasteurization of colostrums and waste milk fed to calves has been shown to reduce the risk of transfer of MAP, is taken up by a number of UK and US dairy farms and may be considered in the future (Stabel, 2001).
Apart from controlling the spread of Johne’s disease it also reduces salmonella spread. Pasteurizing colostrum has also increased the uptake of antibodies into the bloodstream (See calf diarrhea)(Gelsinger et al., 2014)
Findings indicate that wildlife may act as carriers for the disease (Greig et al., 1999). This is unlikely to affect current control strategies, as the logistics of controlling wildlife on grazed pastures is difficult. However, any control strategy should bear in mind additional reservoirs of infection, especially if the farm shares grazing with sheep.
A vaccine which reduces clinical cases and losses is available, but Johne’s disease will not be eradicated by vaccination alone. The vaccine may also interfere with the interpretation of the tuberculin test and any Johne’s antibody testing program. Please consult your vet for further advice.
Treating Johne’s Disease
There is no treatment for Johne’s disease. Animals with confirmed infection should be culled to avoid suffering and to prevent further spread of the disease.
Good Practice Based on Current Knowledge
- Maintain a closed herd and high biosecurity
- Keep cows and their environment clean and free from fecal contamination, especially during the calving period and the first three months of life
- If the herd is Johne’s positive, consider rearing heifers off site, away from adult Johne’s positive cattle
- If animals are bought in, attempt to buy from Johne’s disease monitored herds or test before arrival (a test cannot guarantee freedom from disease)
- In the case of suspected Johne’s disease in the herd, test all animals over 2 years of age and cull positive animals and their offspring
- Do not graze youngstock on ground that has had dung or slurry spread on it until at least a year after application
- Avoid co-grazing youngstock with other livestock that can be infected with Johne’s disease
- In an infected herd, calves should be removed from the dams immediately after birth and given colostrum that is known to be free of the bacteria. In a known infected herd do not pool colostrum for calves as this may spread infection
- Consider joining a Johne’s disease screening and eradication program, such as CHeCS

Comments are closed.